Europe
RefluxStop™ is CE marked in Europe. It is currently available in:
- Germany
- United Kingdom
- Switzerland
- Spain
- Italy
- France
- Austria
- Sweden
- Norway
Follow-on Products
Urology
Implantica’s PotencyFlow® is subject to further development and approval process and is not yet on the market.
Although Viagra type of drugs have improved the situation for the around 300 million men suffering from Erectile Dysfunction, only 50% are able to use these drugs with a successful result.1
PotencyFlow® is designed to treat impotence by controlling blood in the penis during erection.

Pressurized blood causes erection, which may be limited either by too little blood supply to the penis or too much leakage away from the penis. Implantica’s PotencyFlow® is in development to help patients suffering from erectile dysfunction. The device, which is designed to use Implantica’s wireless energy platform, will be controlled wirelessly by a remote control resulting in a smooth chain of events that is expected to lead to a more natural erect penis.
The device is designed to create erection by controlling the blood flow of the penis targeting to treat erectile dysfunction.
The options available today are reconstructive surgery (often with poor long-term result) or a penile implant. Unlike penile implants, PotencyFlow® is designed to not damage the penile erectile tissue and could therefore be preferred entry procedure especially for patients with some functionality left, having vascular problems rather than neurological dysfunction.
PotencyFlow® is intended to be controlled wirelessly resulting in a smooth chain of events that could potentially lead to a more natural erect penis.
Implantica’s solution is designed to target a much larger group of patients than those performing penile implants, due to its additive character, not damaging any remaining functionality of the erection process.
Implantica’s PotencyFlow® is subject to further development and approval process and is not yet on the market.
Wireless control designed to enable activation of erection in a controlled and discrete way.
PotencyFlow® is designed to temporarily control the blood flow and leave the two chambers of the penis (corpora cavernosa) undamaged – unlike current penile implants.
Because PotencyFlow® method of treatment is designed to only be active during a short period of time, the risk of complications could likely be reduced.
Erectile Dysfunction (ED) can be defined as ‘the inability to achieve an erection satisfactory for sexual intercourse. Satisfaction is determined by both patient and partner, making ED a ‘couple’s disease’. The degree of ED can range from a total inability to achieve an erection, an inconsistent ability to do so, or a tendency to sustain only brief erections. The World Health Organization specifies a three-month minimum duration of symptoms to establish the diagnosis. Approximately 5% of 40-year-old men and 15-25% of 65-year old men suffer from complete ED.2
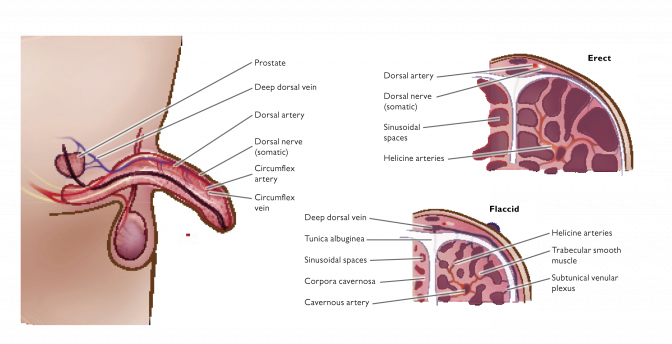
The penis has two chambers called the corpora cavernosa, which run the length of the organ and are filled with spongy tissue. The corpora cavernosa are surrounded by a membrane called the tunica albuginea. The spongy tissue contains smooth muscles, fibrous tissues, spaces, veins and arteries. The urethra runs along the underside of the corpora cavernosa in the corpus spongiosum and is the channel for urine and ejaculate.
An erection is a complex, involuntary, neuropsychological, hormone-mediated, vascular event, which begins with both sensory and mental stimulation. Impulses from the brain and local nerves cause the muscles of the corpora cavernosa to relax, which allows rapid blood flow to fill the spongy chambers, thus creating pressure in the corpora cavernosa and expanding the penis. An erection is sustained when the tunica albuginea helps trap the blood within corpora cavernosa but is reversed when the muscles in the penis contract, which stops the inflow of blood and opens the outflow channels.
Usually, oral drugs are the first step in ED treatment and are referred to as first line treatment. However, these drugs only treat 50% of a group of 300 million men. Penile injection has been used as a second line treatment for over a decade. It has a higher success rate than drug treatment, but it is not generally considered a popular form of treatment with patients because of the need to administer regular self- injection into the corpora cavernosa of the penis.3
Urethral suppositories are another alternative. Following urination, a small pellet is inserted approximately an inch deep into the urethra via an applicator at the tip of the penis. The pellet contains alprostadil. The method is just slightly easier to self-administer than injections and it also suffers from the lack of spontaneity.
Patients generally have tried both drugs and other treatments before they are considered suitable for third line treatment. The use of drugs like Viagra have also caused a rapid increase in the use of penile implants.
Penile prostheses for the treatment of ED have been available for more than 30 years in the US. A key discovery in the field of penile prosthetics was that the corpora cavernosa could be accessed surgically without damaging the penile vessels, urethra or sensory nerves. Intracorporal cylinders can then be installed.4
The most commonly used implants are multi-component inflatable implants, consisting of two or three components. Inflatable cylinders placed in the corpora cavernosa, a fluid reservoir implanted in the abdomen or lower pelvis and a small pump placed in the scrotum. The user squeezes the pump and fluid moves from the reservoir into the cylinders to create an erection. A further squeeze of the pump reverses the process.
The main problem with penile implants is that the normal functionality is damaged permanently, meanwhile a device like PotencyFlow® is designed to add to your exiting functionality.
Implantica is developing products for the treatment of Erectile Dysfunction (ED). The company is focused on high technology products which are being designed to help patients attain a higher quality of life and provide benefits over current existing products with the goal of being easier to use and potentially more acceptable to the patient population.
Formerly known as ‘impotence’, the term Erectile Dysfunction (ED) is now more often used to distinguish it from other problems related with sexual intercourse, e.g. lack of sexual desire or ejaculation and orgasm problems (Brooks & Jordan, 2001). ED is treatable and not a life-threatening disease. However, the condition may result in numerous social and personal problems: depression, withdrawal from sexual intimacy, marital problems, reduced quality of life, decreased working productivity, and increased healthcare utilization (Dhanani et al., 1998, cited by Joyce et al., 2007). With the introduction of Viagra in 1994, the market for erectile dysfunction treatments boomed. Still, many men hesitate to seek help due to the social stigma and embarrassment associated with ED.
Erectile Dysfunction was defined at the National Institutes of Health Consensus Conference in Washington DC, US, December 1992 as ‘the inability to achieve an erection satisfactory for sexual intercourse’ (National Institutes of Health, 1993). Satisfaction is determined by both patient and partner, making ED a ‘couple’s disease’. The degree of ED can range from a total inability to achieve an erection, an inconsistent ability to do so, or a tendency to sustain only brief erections. The World Health Organization specifies a three-month minimum duration of symptoms to establish the diagnosis (WHO cited by Joyce et al., 2007).
Approximately 5 % of 40 year old men and 15-25 % of 65 year old men suffer from complete ED (Brooks & Jordan, 2001; NKUIDC, 2007).
The penis has two chambers called the corpora cavernosa, which run the length of the organ and are filled with spongy tissue. The corpora cavernosa are surrounded by a membrane called the tunica albuginea. The spongy tissue contains smooth muscles, fibrous tissues, spaces, veins and arteries. The urethra runs along the underside of the corpora cavernosa in the corpus spongiosum and is the channel for urine and ejaculate.
An erection is a complex, involuntary, neuropsychological, hormone-mediated, vascular event, which begins with both sensory and mental stimulation. Impulses from the brain and local nerves cause the muscles of the corpora cavernosa to relax, which allows rapid blood flow to fill the spongy chambers, thus creating pressure in the corpora cavernosa and expanding the penis. An erection is sustained when the tunica albuginea helps trap the blood within corpora cavernosa but is reversed when the muscles in the penis contract, which stops the inflow of blood and opens the outflow channels.
As previously mentioned, there is a well-defined sequence of events that take place to enable an erection. ED can occur when any of these events are disrupted. Brooks & Jordan (2001) states the cause in more than 75 % of the cases is physical rather than psychological and that the most common cause is damage either to arteries, smooth muscles or fibrous tissues and those damages accounts for approximately 70 % of the cases.