Europe
RefluxStop™ is CE marked in Europe. It is currently available in:
- Germany
- United Kingdom
- Switzerland
- Spain
- Italy
- France
- Austria
- Sweden
- Norway
Follow-on Products
eHealth
Implantica’s AneurysmControl™ is subject to further development and approval process and is not yet on the market. An aortic aneurysm is an abnormal bulge that occurs in the wall of a blood vessel. It may occur in the brain of young people, but is most often located in the major blood vessel (aorta) that carries blood from your heart to your body. It affects more men than women and up to 8% of men above 60 years old1. Larger aortic aneurysms could suddenly start to expand and burst, with potentially deadly consequences. More people die from this disease than from car accidents, in the US the magnitude of 28’000 people died from this disease in 2009. Therefore, a large screening program has been started all over the world. Due to the high-risk surgery only the largest sizes above 5,5 cm are operated, which is about 15% of the patients found during the screening process.
AneurysmControl™ is designed to target to save lives by monitoring the expansion of the aneurysm.

Implantica’s AneurysmControl™ is designed to be a preventive method to control and treat the aneurysm also in earlier stages, with the intended result that emergency operations and sudden deaths can be avoided.
Patients not operated are followed by ultrasound investigation every 3-6 months. AneurysmControl™ is designed with the intention to continuously monitor the aneurysm, estimated to make regular, costly and time consuming ultrasonography unnecessary, which is the current standard monitoring approach following the detection of an aneurysm. In addition, currently only later-stage aneurysms can be treated, whereas AneurysmControl™ is designed with the potential to be able to treat and monitor aneurysms at any stage.
AneurysmControl™ is designed with the intention to treat and monitor up to 80% of the patients identified as at risk through worldwide screening programs.
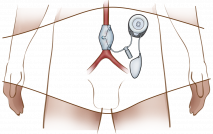
The innovative solution is designed to use a pressure-calibrated hydraulic cuff, which is intended to help to slow down or prevent further expansion of the aneurysm. At the same time, the device is designed to monitor the change in size of the aneurysm to inform the Patient and the Caregiver – an innovative and important feature. The hydraulic system is designed to exert constant light pressure against the aneurysm with the ability to increase the pressure automatically if expansion should occur. AneurysmControl™ is designed with the intention to also prevent further expansion of the aneurysm as well as monitor it, to avoid both future aneurysm rupture with high risk of death and later highly risky surgery.
AneurysmControl™ is designed to protect a growing aneurysm from rupture with a hydraulic support.
AneurysmControl™ is designed to continuously monitor the growth of the aneurysm, thereby, targeting reducing patient risk. If an aneurysm would start to expand the smart implant is designed to automatically increase the contra pressure on the aneurysm to avoid self-expansion and death.
Because of the increased use of ultrasound screening of patients at risk of developing aortic aneurysm, it will be possible to identify patients in an early stage of the disease. AneurysmControl™ is intended to be the only product on the market to treat this group of patients.
The large number of deaths caused by Aorta aneurysm motivates use of early protection implants such as AneurysmControl™. Benefits of early protection and monitoring of the aneurysm target to avoid self-expansion and bursting aneurysms causing deaths, outweigh the risks associated with a surgical procedure.
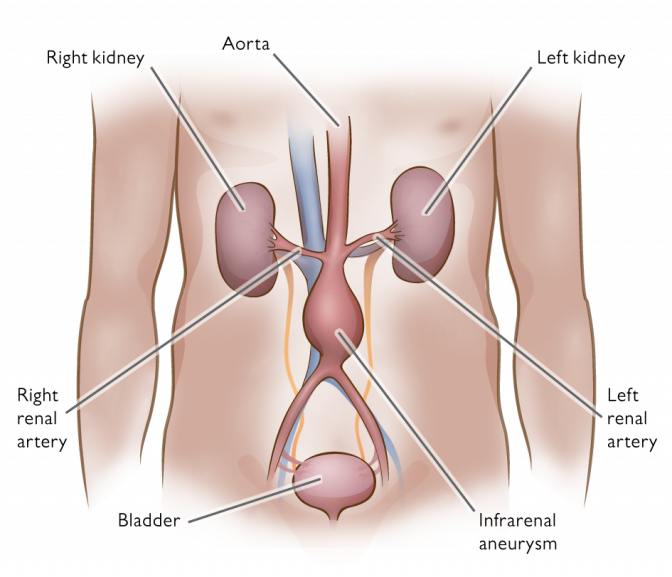
An aneurysm is an abnormal bulging or swelling of a portion of a blood vessel. The aorta, which can develop these abnormal bulges, is the large blood vessel that carries oxygen-rich blood away from the heart to the rest of the body. Aorta aneurysm usually occurs in the abdomen below the kidneys (abdominal aortic aneurysm) but may occur in the chest cavity (thoracic aortic aneurysm).
Aorta aneurysm falls under the broader term cardiovascular disease which is used to describe a range of diseases that affect the heart and blood vessels of the human circulatory system. If untreated, an aneurysm may rupture, resulting in internal bleeding. A large rupture may be rapidly fatal.
As mentioned, in order to prevent deaths, large screening programs have started all over the world to find specifically aortic aneurysms. These aneurysms cause more deaths than traffic accidents Abdominal aortic aneurysm is found in up to 8% of men1 more than 60 years old, and while it is less common among women, studies have shown that women have a worse prognosis than men.
Currently, early stage aneurysms often go untreated. Instead, small aneurysms are monitored for their rate of growth and only large aneurysms are treated.
Small aneurysms are deemed small when the risk of repair exceeds the risk of rupture, usually aneurysms with a diameter of less than 5 cm. Today, these are monitored by performing ultrasonography every 3 to 6 months.
When an abdominal aortic aneurysm, the most common form of aneurysm, is judged to be large enough to carry risk of rupture, there are two types of surgery performed, however, due to high risk only considered for about the 15% of the patients with the largest aneurysms. However, also smaller aneurysm could start to self expand and rupture. It does not fully help to perform an ultrasound every 3-6 months when an expansion could occur very rapidly anytime, however, no other treatment exists today. Therefore AneurysmControlTM has been designedwith the intention to save lives and monitor the aneurysms not operated, however, please observe it is subject to further development and approval process and is not yet on the market.
The two prevailing surgical solutions today are; a) replacing the aneurysm with an artificial blood vessel using a synthetic graft to repair the aneurysm and b) endovascular repair (EVAR) using a large stent to place inside the aneurysm in the blood vessel. Both of these procedures carry high risk and are only used for the largest aneurysms. The risk of death during an emergency repair of a ruptured aneurysm is about 50%2.
Aortic aneurysm can develop anywhere in the aorta. The more common form of aortic aneurysm is abdominal aortic aneurysm (AAA) that is a localized dilatation (bulge) of the abdominal aorta that exceeds the normal diameter by more than 50%. The normal diameter of infrarenal aorta is 2 cm. Aneurysm is caused by a degenerative process of the aortic wall most commonly located infrarenally. The pressure of blood inside the artery forces the weak area to balloon outward. If untreated, an aneurysm may rupture, resulting in internal bleeding. Aortic aneurysms are potentially life-threatening conditions. If the aneurysm is untreated and eventually ruptures, it can lead to death.
Small aneurysms should be monitored for their rate of growth and large aneurysms require consideration for a surgical repair.
The treatment options for the more common form of aneurysm, abdominal aortic aneurysm (AAA), are employed in accordance to their different indications:
Endovascular repair (EVAR) is generally indicated in older, high risk patients or patients unfit for open repair. EVAR is less invasive approach than open surgery. In EVAR, mostly stented grafts are used and placed in the aneurismal area of the aorta. Endovascular repair is feasible for only a proportion of abdominal aortic aneurysms, depending on the morphology of the aneurysm.
As knowledge increases about the prevalence of vascular disorders, health care providers and government leaders have become more aware of the economic burden of these conditions.
Cardiovascular-related disease generates more healthcare costs and lost income than most other therapeutic areas. The cost is accelerating as the population ages and expands, creating unprecedented demand for new effective treatments that prevent, delay and cure vascular-related illnesses.
Cardiovascular disease can lead to aortic aneurysm, a significant and life-threatening condition. Implantica is currently developing new technologies which will be used in the treatment of this condition. AneurysmControl™ is designed with the intention to provide increased life expectancy and decreased mortality.